The  MyoVision
system allows the objective quantification and documentation of spinal pain and soft tissue injury.
The MyoVision system was developed by a NASA-trained scientist, and is considered the "gold standard" by the
American Medical Association; it has also been acknowledged as valid by the Florida Supreme Court.
MyoVision
system allows the objective quantification and documentation of spinal pain and soft tissue injury.
The MyoVision system was developed by a NASA-trained scientist, and is considered the "gold standard" by the
American Medical Association; it has also been acknowledged as valid by the Florida Supreme Court.
It helps provide answers to questions like:
- The patient's MRI, CT, and X-rays are normal - What proof is there that the patient is really in pain?
- The patient's range of motion (ROM) is normal - what proof is there that the patient is functionally impaired?
- Does the patient have a Personal Injury (PI) or Workman's Compensation (WC) case?
- Is the current treatment protocol helping the patient, or has the patient achieved "Maximal Medical Improvement (MMI)?
- Does the patient have a permanent disability?
- For patients engaging in hazardous activities (sports, military service, etc), what is their baseline that future injuries can be compared against?
This information is essential to doctors and patients who need to objectively document, when combined with appropriate clinical testing, to third party payors (insurance companies, workman's comp, medical examiners, etc) the best plan for further treatment, or that no further treatment is indicated.
How it Works
 The MyoVision system works by combining dynamic measurement of joint motion using two inclinometers
(round black instruments in illustration) with simultaneous
dynamic measurements (in microvolts) of paraspinal
and/or sternocleidomastoid muscle activity (red and white wires in illustration).
This surface electromyogram works in the same way as recording of cardiac muscle contractions in microvolts
with ECG.
The MyoVision system works by combining dynamic measurement of joint motion using two inclinometers
(round black instruments in illustration) with simultaneous
dynamic measurements (in microvolts) of paraspinal
and/or sternocleidomastoid muscle activity (red and white wires in illustration).
This surface electromyogram works in the same way as recording of cardiac muscle contractions in microvolts
with ECG.
Shown here, lumbar flexion is being studied. Both cervical and lumbar flexion, extension, lateral flexion, and rotation are included in the complete test sequence.
The graphical presentation of the results provides
definitive evidence of ligament pain resulting in muscle guarding, fasciculations,
and/or abnormal muscle recruitment that cannot be "faked",
thereby providing insight into the nature of the currently remaining problems.
Interpretation of Results
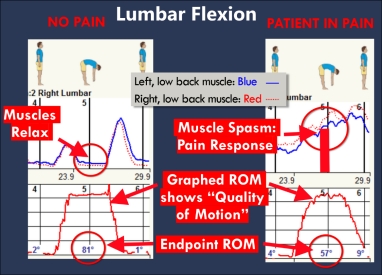 The normal data presentation for lumbar flexion is shown on the left - notice the smooth trace of muscle activity on the top left,
and in particular that at end of range (full flexion), muscle activity drops to baseline as the torso is supported by ligaments rather than muscles.
Also note the smooth, crisp trace of range of motion in the lower left trace.
On the other hand, in the upper right trace, objective evidence of pain includes the jagged trace of muscle activity that does not drop to baseline at full flexion,
although the range of motion obtained (bottom right) is very nearly the same as the normal case.
The normal data presentation for lumbar flexion is shown on the left - notice the smooth trace of muscle activity on the top left,
and in particular that at end of range (full flexion), muscle activity drops to baseline as the torso is supported by ligaments rather than muscles.
Also note the smooth, crisp trace of range of motion in the lower left trace.
On the other hand, in the upper right trace, objective evidence of pain includes the jagged trace of muscle activity that does not drop to baseline at full flexion,
although the range of motion obtained (bottom right) is very nearly the same as the normal case.
Theory
Pain experienced in motion leads to a muscular response commonly known as spasm, hypertonicity, or muscle guarding; studies have found that the simultaneous measurement of muscle guarding along with range of motion increases sensitivity and specificity of range of motion to pain [Geisser2005]. Muscle guarding is the body's natural defense mechanism in response to pain, and the DynaROM system objectively quantifies this muscular guarding in motion. This muscle guarding corresponds to 5-8% impairment in the AMA Permanent Guides to Impairment (5th edition).
On the other hand, range of motion on its own is a poor indicator of pain, as many patients have normal range of motion concomitant with significant muscle guarding and pain.
Unlike needle EMG, which is used to evaluate for nerve damage by looking at a single motor neuron, the DynaROM measures the region's response to pain by objectively measuring globally the involved region's (e.g. lumbar paraspinal muscles) response to pain. The graphical presentation of the results provides definitive evidence of pain (muscle guarding, fasciculations, ratcheting, and abnormal muscle recruitment) that cannot be "faked", and provides insight into the nature of the remaining problems.
Cost
Complete MyoVision testing of cervical and lumbar flexion, extension, lateral flexion, and rotation, including a color print-out of the data and a 15 minute oral review is $75, while a written interpretive report is an additional $150, payable at time of service (no contingency or liens accepted).